Uterine Sarcoma Treatment (PDQ®): Treatment – Patient Information [NCI]
General Information About Uterine Sarcoma
Uterine sarcoma is a disease in which malignant (cancer) cells form in the muscles of the uterus or other tissues that support the uterus.
The uterus is part of the female reproductive system. The uterus is the hollow, pear-shaped organ in the pelvis, where a fetus grows. The cervix is at the lower, narrow end of the uterus, and leads to the vagina. 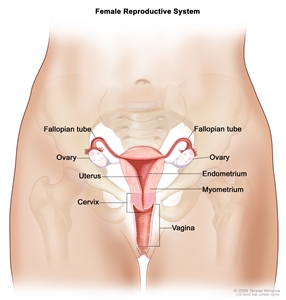
Anatomy of the female reproductive system. The organs in the female reproductive system include the uterus, ovaries, fallopian tubes, cervix, and vagina. The uterus has a muscular outer layer called the myometrium and an inner lining called the endometrium.
Uterine sarcoma is a very rare kind of cancer that forms in the uterine muscles or in tissues that support the uterus. (Information about other types of sarcomas can be found in the PDQ summary on Adult Soft Tissue Sarcoma Treatment.) Uterine sarcoma is different from cancer of the endometrium, a disease in which cancer cells start growing inside the lining of the uterus. (See the PDQ summary on Endometrial Cancer Treatment for information).
Past treatment with radiation therapy to the pelvis can increase the risk of uterine sarcoma.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk. Risk factors for uterine sarcoma include the following:
- Past treatment with radiation therapy to the pelvis.
- Treatment with tamoxifen for breast cancer. If you are taking this drug, have a pelvic exam every year and report any vaginal bleeding (other than menstrual bleeding) as soon as possible.
Signs of uterine sarcoma include abnormal bleeding.
Abnormal bleeding from the vagina and other signs and symptoms may be caused by uterine sarcoma or by other conditions. Check with your doctor if you have any of the following:
- Bleeding that is not part of menstrual periods.
- Bleeding after menopause.
- A mass in the vagina.
- Pain or a feeling of fullness in the abdomen.
- Frequent urination.
Tests that examine the uterus are used to detect (find) and diagnose uterine sarcoma.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Pelvic exam: An exam of the vagina, cervix, uterus, fallopian tubes, ovaries, and rectum. A speculum is inserted into the vagina and the doctor or nurse looks at the vagina and cervix for signs of disease. A Pap test of the cervix is usually done. The doctor or nurse also inserts one or two lubricated, gloved fingers of one hand into the vagina and places the other hand over the lower abdomen to feel the size, shape, and position of the uterus and ovaries. The doctor or nurse also inserts a lubricated, gloved finger into the rectum to feel for lumps or abnormal areas.
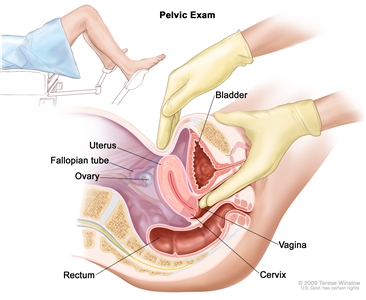
Pelvic exam. A doctor or nurse inserts one or two lubricated, gloved fingers of one hand into the vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked. - Pap test: A procedure to collect cells from the surface of the cervix and vagina. A piece of cotton, a brush, or a small wooden stick is used to gently scrape cells from the cervix and vagina. The cells are viewed under a microscope to find out if they are abnormal. This procedure is also called a Pap smear. Because uterine sarcoma begins inside the uterus, this cancer may not show up on the Pap test.
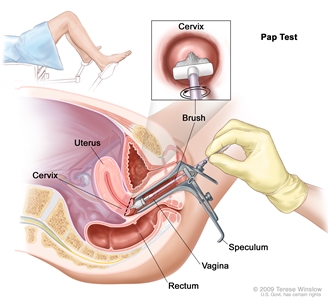
Pap test. A speculum is inserted into the vagina to widen it. Then, a brush is inserted into the vagina to collect cells from the cervix. The cells are checked under a microscope for signs of disease. - Transvaginal ultrasound exam: A procedure used to examine the vagina, uterus, fallopian tubes, and bladder. An ultrasound transducer (probe) is inserted into the vagina and used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The doctor can identify tumors by looking at the sonogram.
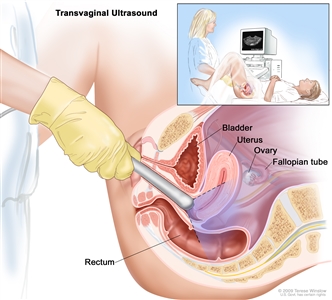
Transvaginal ultrasound. An ultrasound probe connected to a computer is inserted into the vagina and is gently moved to show different organs. The probe bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture). - Dilatation and curettage: A procedure to remove samples of tissue from the inner lining of the uterus. The cervix is dilated and a curette (spoon-shaped instrument) is inserted into the uterus to remove tissue. The tissue samples are checked under a microscope for signs of disease. This procedure is also called a D&C.
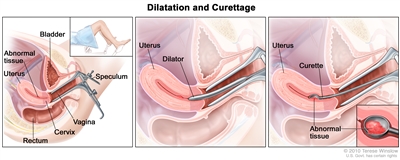
Dilatation and curettage (D and C). A speculum is inserted into the vagina to widen it in order to look at the cervix (first panel). A dilator is used to widen the cervix (middle panel). A curette is put through the cervix into the uterus to scrape out abnormal tissue (last panel). - Endometrial biopsy: The removal of tissue from the endometrium (inner lining of the uterus) by inserting a thin, flexible tube through the cervix and into the uterus. The tube is used to gently scrape a small amount of tissue from the endometrium and then remove the tissue samples. A pathologist views the tissue under a microscope to look for cancer cells.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer.
- The type and size of the tumor.
- The patient’s general health.
- Whether the cancer has just been diagnosed or has recurred (come back).
Stages of Uterine Sarcoma
After uterine sarcoma has been diagnosed, tests are done to find out if cancer cells have spread within the uterus or to other parts of the body.
The process used to find out if cancer has spread within the uterus or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The following procedures may be used in the staging process:
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- CA 125 assay: A test that measures the level of CA 125 in the blood. CA 125 is a substance released by cells into the bloodstream. An increased CA 125 level is sometimes a sign of cancer or other condition.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Transvaginal ultrasound exam: A procedure used to examine the vagina, uterus, fallopian tubes, and bladder. An ultrasound transducer (probe) is inserted into the vagina and used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The doctor can identify tumors by looking at the sonogram.
Transvaginal ultrasound. An ultrasound probe connected to a computer is inserted into the vagina and is gently moved to show different organs. The probe bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture). - CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the abdomen and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues to show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Cystoscopy: A procedure to look inside the bladder and urethra to check for abnormal areas. A cystoscope is inserted through the urethra into the bladder. A cystoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
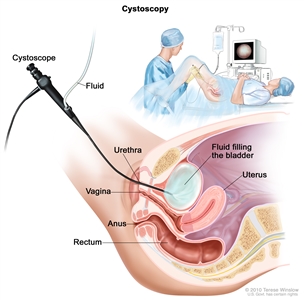
Cystoscopy. A cystoscope (a thin, tube-like instrument with a light and a lens for viewing) is inserted through the urethra into the bladder. Fluid is used to fill the bladder. The doctor looks at an image of the inner wall of the bladder on a computer monitor.
Uterine sarcoma may be diagnosed, staged, and treated in the same surgery.
Surgery is used to diagnose, stage, and treat uterine sarcoma. During this surgery, the doctor removes as much of the cancer as possible. The following procedures may be used to diagnose, stage, and treat uterine sarcoma:
- Laparotomy: A surgical procedure in which an incision (cut) is made in the wall of the abdomen to check the inside of the abdomen for signs of disease. The size of the incision depends on the reason the laparotomy is being done. Sometimes organs are removed or tissue samples are taken and checked under a microscope for signs of disease.
- Abdominal and pelvic washings: A procedure in which a saline solution is placed into the abdominal and pelvic body cavities. After a short time, the fluid is removed and viewed under a microscope to check for cancer cells.
- Total abdominal hysterectomy: A surgical procedure to remove the uterus and cervix through a large incision (cut) in the abdomen.
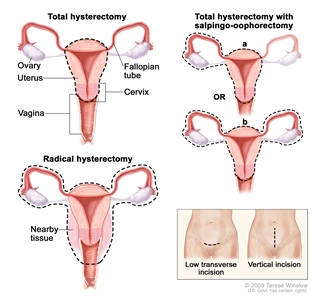
Hysterectomy. The uterus is surgically removed with or without other organs or tissues. In a total hysterectomy, the uterus and cervix are removed. In a total hysterectomy with salpingo-oophorectomy, (a) the uterus plus one (unilateral) ovary and fallopian tube are removed; or (b) the uterus plus both (bilateral) ovaries and fallopian tubes are removed. In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision. - Bilateral salpingo-oophorectomy: Surgery to remove both ovaries and both fallopian tubes.
- Lymphadenectomy: A surgical procedure in which lymph nodes are removed and checked under a microscope for signs of cancer. For a regional lymphadenectomy, some of the lymph nodes in the tumor area are removed. For a radical lymphadenectomy, most or all of the lymph nodes in the tumor area are removed. This procedure is also called lymph node dissection.
Treatment in addition to surgery may be given, as described in the Treatment Option Overview section of this summary.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if uterine sarcoma spreads to the lung, the cancer cells in the lung are actually uterine sarcoma cells. The disease is metastatic uterine sarcoma, not lung cancer.
The following stages are used for uterine sarcoma:
Stage I
In stage I, cancer is found in the uterus only. Stage I is divided into stages IA and IB, based on how far the cancer has spread.
- Stage IA: Cancer is in the endometrium only or less than halfway through the myometrium (muscle layer of the uterus).
- Stage IB: Cancer has spread halfway or more into the myometrium.
Stage II
In stage II, cancer has spread into connective tissue of the cervix, but has not spread outside the uterus.
Stage III
In stage III, cancer has spread beyond the uterus and cervix, but has not spread beyond the pelvis. Stage III is divided into stages IIIA, IIIB, and IIIC, based on how far the cancer has spread within the pelvis.
- Stage IIIA: Cancer has spread to the outer layer of the uterus and/or to the fallopian tubes, ovaries, and ligaments of the uterus.
- Stage IIIB: Cancer has spread to the vagina or to the parametrium (connective tissue and fat around the uterus).
- Stage IIIC: Cancer has spread to lymph nodes in the pelvis and/or around the aorta (largest artery in the body, which carries blood away from the heart).
Stage IV
In stage IV, cancer has spread beyond the pelvis. Stage IV is divided into stages IVA and IVB, based on how far the cancer has spread.
- Stage IVA: Cancer has spread to the bladder and/or bowel wall.
- Stage IVB: Cancer has spread to other parts of the body beyond the pelvis, including the abdomen and/or lymph nodes in the groin.