Gastric Cancer Treatment (PDQ®): Treatment – Patient Information [NCI]
General Information About Gastric Cancer
Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach.
The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive system, which processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) in foods that are eaten and helps pass waste material out of the body. Food moves from the throat to the stomach through a hollow, muscular tube called the esophagus. After leaving the stomach, partly-digested food passes into the small intestine and then into the large intestine. 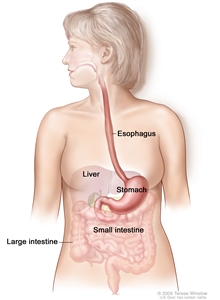
The esophagus and stomach are part of the upper gastrointestinal (digestive) system.
The wall of the stomach is made up of 5 layers of tissue. From the innermost layer to the outermost layer, the layers of the stomach wall are: mucosa, submucosa, muscle, subserosa (connective tissue), and serosa. Gastric cancer begins in the mucosa and spreads through the outer layers as it grows.
Stromal tumors of the stomach begin in supporting connective tissue and are treated differently from gastric cancer. See the PDQ summary on Gastrointestinal Stromal Tumors Treatment for more information.
For more information about cancers of the stomach, see the following PDQ summaries:
- Unusual Cancers of Childhood Treatment
- Stomach (Gastric) Cancer Prevention
- Stomach (Gastric) Cancer Screening
Age, diet, and stomach disease can affect the risk of developing gastric cancer.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk. Risk factors for gastric cancer include the following:
- Having any of the following medical conditions:
- Helicobacter pylori (H. pylori) infection of the stomach.
- Chronic gastritis (inflammation of the stomach).
- Pernicious anemia.
- Intestinal metaplasia (a condition in which the normal stomach lining is replaced with the cells that line the intestines).
- Gastric polyps.
- Epstein-Barr virus.
- Familial syndromes (including familial adenomatous polyposis).
- Eating a diet high in salted, smoked foods and low in fruits and vegetables.
- Eating foods that have not been prepared or stored properly.
- Being older or male.
- Smoking cigarettes.
- Having a mother, father, sister, or brother who has had stomach cancer.
Symptoms of gastric cancer include indigestion and stomach discomfort or pain.
These and other signs and symptoms may be caused by gastric cancer or by other conditions.
In the early stages of gastric cancer, the following symptoms may occur:
- Indigestion and stomach discomfort.
- A bloated feeling after eating.
- Mild nausea.
- Loss of appetite.
- Heartburn.
In more advanced stages of gastric cancer, the following signs and symptoms may occur:
- Blood in the stool.
- Vomiting.
- Weight loss for no known reason.
- Stomach pain.
- Jaundice (yellowing of eyes and skin).
- Ascites (build-up of fluid in the abdomen).
- Trouble swallowing.
Check with your doctor if you have any of these problems.
Tests that examine the stomach and esophagus are used to detect (find) and diagnose gastric cancer.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Complete blood count (CBC): A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells, white blood cells, and platelets.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the sample made up of red blood cells.
- Upper endoscopy: A procedure to look inside the esophagus, stomach, and duodenum (first part of the small intestine) to check for abnormal areas. An endoscope (a thin, lighted tube) is passed through the mouth and down the throat into the esophagus.
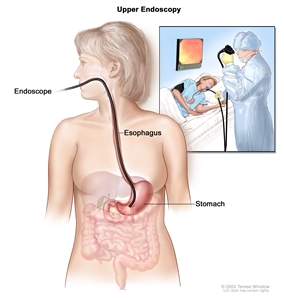
Upper endoscopy. A thin, lighted tube is inserted through the mouth to look for abnormal areas in the esophagus, stomach, and first part of the small intestine. - Barium swallow: A series of x-rays of the esophagus and stomach. The patient drinks a liquid that contains barium (a silver-white metallic compound). The liquid coats the esophagus and stomach, and x-rays are taken. This procedure is also called an upper GI series.
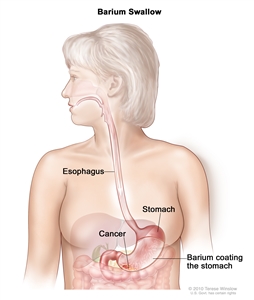
Barium swallow for stomach cancer. The patient swallows barium liquid and it flows through the esophagus and into the stomach. X-rays are taken to look for abnormal areas. - CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. A biopsy of the stomach is usually done during the endoscopy.
The sample of tissue may be checked to measure how many HER2genes there are and how much HER2 protein is being made. If there are more HER2 genes or higher levels of HER2 protein than normal, the cancer is called HER2 positive. HER2-positive gastric cancer may be treated with a monoclonal antibody that targets the HER2 protein.
The sample of tissue may also be checked for Helicobacter pylori (H. pylori) infection.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer (whether it is in the stomach only or has spread to lymph nodes or other places in the body).
- The patient’s general health.
When gastric cancer is found very early, there is a better chance of recovery. Gastric cancer is often in an advanced stage when it is diagnosed. At later stages, gastric cancer can be treated but rarely can be cured. Taking part in one of the clinical trials being done to improve treatment should be considered. Information about ongoing clinical trials is available from the NCI website.
Stages of Gastric Cancer
After gastric cancer has been diagnosed, tests are done to find out if cancer cells have spread within the stomach or to other parts of the body.
The process used to find out if cancer has spread within the stomach or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used in the staging process:
- Endoscopic ultrasound (EUS): A procedure in which an endoscope is inserted into the body, usually through the mouth or rectum. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest, abdomen, or pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. A PET scan and CT scan may be done at the same time. This is called a PET-CT.
- MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Laparoscopy: A surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples to be checked under a microscope for signs of cancer. A solution may be washed over the surface of the organs in the abdomen and then removed to collect cells. These cells are also looked at under a microscope to check for signs of cancer.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if gastric cancer spreads to the liver, the cancer cells in the liver are actually gastric cancer cells. The disease is metastatic gastric cancer, not liver cancer.
The following stages are used for gastric cancer:
Stage 0 (Carcinoma in Situ)
In stage 0, abnormal cells are found in the mucosa (innermost layer) of the stomach wall. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
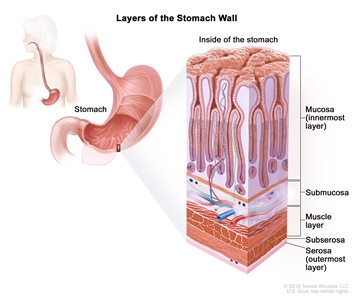
Layers of the stomach wall. The wall of the stomach is made up of the mucosa (innermost layer), submucosa, muscle layer, subserosa, and serosa (outermost layer). The stomach is an organ in the upper abdomen.
Stage I
Stage I is divided into stages IA and IB.
- Stage IA: Cancer has formed in the mucosa (innermost layer) of the stomach wall and may have spread to the submucosa (layer of tissue next to the mucosa).
- Stage IB: Cancer:
- has formed in the mucosa (innermost layer) of the stomach wall and may have spread to the submucosa (layer of tissue next to the mucosa). Cancer has spread to 1 or 2 nearby lymph nodes; or
- has formed in the mucosa of the stomach wall and has spread to the muscle layer.
Stage II
Stage II gastric cancer is divided into stages IIA and IIB.
- Stage IIA: Cancer:
- may have spread to the submucosa (layer of tissue next to the mucosa) of the stomach wall. Cancer has spread to 3 to 6 nearby lymph nodes; or
- has spread to the muscle layer of the stomach wall. Cancer has spread to 1 or 2 nearby lymph nodes; or
- has spread to the subserosa (layer of connective tissue next to the muscle layer) of the stomach wall.
- Stage IIB: Cancer:
- may have spread to the submucosa (layer of tissue next to the mucosa) of the stomach wall. Cancer has spread to 7 to 15 nearby lymph nodes; or
- has spread to the muscle layer of the stomach wall. Cancer has spread to 3 to 6 nearby lymph nodes; or
- has spread to the subserosa (layer of connective tissue next to the muscle layer) of the stomach wall. Cancer has spread to 1 or 2 nearby lymph nodes; or
- has spread to the serosa (outermost layer) of the stomach wall.
Stage III
Stage III gastric cancer is divided into stages IIIA, IIIB, and IIIC.
- Stage IIIA: Cancer has spread:
- to the muscle layer of the stomach wall. Cancer has spread to 7 to 15 nearby lymph nodes; or
- to the subserosa (layer of connective tissue next to the muscle layer) of the stomach wall. Cancer has spread to 3 to 6 nearby lymph nodes; or
- to the serosa (outermost layer) of the stomach wall. Cancer has spread to 1 to 6 nearby lymph nodes; or
- to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen.
- Stage IIIB: Cancer:
- may have spread to the submucosa (layer of tissue next to the mucosa) or to the muscle layer of the stomach wall. Cancer has spread to 16 or more nearby lymph nodes; or
- has spread to the subserosa (layer of connective tissue next to the muscle layer) or to the serosa (outermost layer) of the stomach wall. Cancer has spread to 7 to 15 nearby lymph nodes; or
- has spread from the stomach to nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen. Cancer has spread to 1 to 6 nearby lymph nodes.
- Stage IIIC: Cancer has spread:
- to the subserosa (layer of connective tissue next to the muscle layer) or to the serosa (outermost layer) of the stomach wall. Cancer has spread to 16 or more nearby lymph nodes; or
- from the stomach into nearby organs, such as the spleen, colon, liver, diaphragm, pancreas, abdomen wall, adrenal gland, kidney, or small intestine, or to the back of the abdomen. Cancer has spread to 7 or more nearby lymph nodes.
Stage IV
In stage IV, cancer has spread to other parts of the body, such as the lungs, liver, distant lymph nodes, and the tissue that lines the abdomen wall.
Treatment Option Overview
There are different types of treatment for patients with gastric cancer.
Different types of treatments are available for patients with gastric cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Seven types of standard treatment are used:
Surgery
Surgery is a common treatment of all stages of gastric cancer. The following types of surgery may be used:
- Subtotal gastrectomy: Removal of the part of the stomach that contains cancer, nearby lymph nodes, and parts of other tissues and organs near the tumor. The spleen may be removed. The spleen is an organ that makes lymphocytes, stores red blood cells and lymphocytes, filters the blood, and destroys old blood cells. The spleen is on the left side of the abdomen near the stomach.
- Total gastrectomy: Removal of the entire stomach, nearby lymph nodes, and parts of the esophagus, small intestine, and other tissues near the tumor. The spleen may be removed. The esophagus is connected to the small intestine so the patient can continue to eat and swallow.
If the tumor is blocking the stomach but the cancer cannot be completely removed by standard surgery, the following procedures may be used:
- Endoluminal stent placement: A procedure to insert a stent (a thin, expandable tube) in order to keep a passage (such as arteries or the esophagus) open. For tumors blocking the passage into or out of the stomach, surgery may be done to place a stent from the esophagus to the stomach or from the stomach to the small intestine to allow the patient to eat normally.
- Endoluminal laser therapy: A procedure in which an endoscope (a thin, lighted tube) with a laser attached is inserted into the body. A laser is an intense beam of light that can be used as a knife.
- Gastrojejunostomy: Surgery to remove the part of the stomach with cancer that is blocking the opening into the small intestine. The stomach is connected to the jejunum (a part of the small intestine) to allow food and medicine to pass from the stomach into the small intestine.
Endoscopic mucosal resection
Endoscopic mucosal resection is a procedure that uses an endoscope to remove early-stage cancer and precancerous growths from the lining of the digestive tract without surgery. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also include tools to remove growths from the lining of the digestive tract.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
A type of regional chemotherapy being studied to treat gastric cancer is intraperitoneal (IP) chemotherapy. In IP chemotherapy, the anticancer drugs are carried directly into the peritoneal cavity (the space that contains the abdominal organs) through a thin tube.
Hyperthermic intraperitoneal chemotherapy (HIPEC) is a treatment used during surgery that is being studied for gastric cancer. After the surgeon has removed as much tumor tissue as possible, warmed chemotherapy is sent directly into the peritoneal cavity.
See Drugs Approved for Stomach (Gastric) Cancer for more information.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External radiation therapy is used to treat gastric cancer.
Chemoradiation
Chemoradiation therapy combines chemotherapy and radiation therapy to increase the effects of both. Chemoradiation given after surgery, to lower the risk that the cancer will come back, is called adjuvant therapy. Chemoradiation given before surgery, to shrink the tumor (neoadjuvant therapy), is being studied.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Monoclonal antibodies and multikinase inhibitors are types of targeted therapy used in the treatment of gastric cancer.
- Monoclonal antibody therapy: This type of therapy uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
There are different types of monoclonal antibody drugs:
- Trastuzumab blocks the effect of the growth factor protein HER2, which sends growth signals to gastric cancer cells.
- Ramucirumab blocks the effect of certain proteins, including vascular endothelial growth factor. This may help keep cancer cells from growing and may kill them. It may also prevent the growth of new blood vessels that tumors need to grow.
Trastuzumab and ramucirumab are used in the treatment of stage IV gastric cancer and gastric cancer that cannot be removed by surgery or has recurred.
- Multikinase inhibitors: These are small-molecule drugs that go through the cell membrane and work inside cancer cells to block multiple protein signals that cancer cells need to grow and divide. Some multikinase inhibitors also have angiogenesis inhibitor effects. Angiogenesis inhibitors stop the growth of new blood vessels that tumors need to grow.
There are different types of multikinase inhibitor drugs:
- Regorafenib is a multikinase inhibitor and angiogenesis inhibitor that blocks the effects of the multiple proteins inside tumor cells. Regorafenib is being studied in the treatment of stage IV gastric cancer and gastric cancer that cannot be removed by surgery or has recurred.
See Drugs Approved for Stomach (Gastric) Cancer for more information.
Immunotherapy
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. This type of cancer treatment is also called biotherapy or biologic therapy.
Immune checkpoint inhibitor therapy is a type of immunotherapy.
- Immune checkpoint inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. When PD-1 attaches to another protein called PDL-1 on a cancer cell, it stops the T cell from killing the cancer cell. PD-1 inhibitors attach to PDL-1 and allow the T cells to kill cancer cells. Pembrolizumab is a type of immune checkpoint inhibitor.
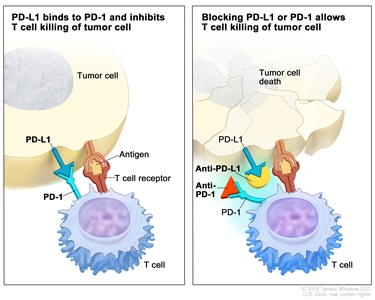
Immune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
See Drugs Approved for Stomach (Gastric) Cancer for more information.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for gastric cancer may cause side effects.
For information about side effects caused by treatment for cancer, see our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Other tests may also be done:
- Carcinoembryonic antigen (CEA) assay and CA 19-9 assay: A procedure in which a sample tissue is checked to measure the amounts of certain substances made by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the body. These are called tumor markers. Higher than normal levels of carcinoembryonic antigen (CEA) and CA 19-9 may mean gastric cancer has come back after treatment.