Thoracentesis
Test Overview
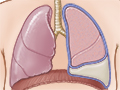
Thoracentesis is a procedure to remove fluid from the space between the lungs and the chest wall called the pleural space. It is done with a needle (and sometimes a plastic catheter) inserted through the chest wall. Ultrasound pictures are often used to guide the placement of the needle. This pleural fluid may be sent to a lab to determine what may be causing the fluid to build up in the pleural space.
Normally only a small amount of pleural fluid is present in the pleural space. A buildup of excess pleural fluid (pleural effusion) may be caused by many conditions, such as infection, inflammation, heart failure, or cancer. If a large amount of fluid is present, it may be hard to breathe. Fluid inside the pleural space may be found during a physical examination and is usually confirmed by a chest X-ray.
Why It Is Done
Thoracentesis may be done to:
- Find the cause of excess pleural fluid (pleural effusion).
- Relieve shortness of breath and pain caused by a pleural effusion.
How To Prepare
You will be asked to sign a consent form that says you understand the risks of the test and agree to have it done.
Talk to your doctor about any concerns you have regarding the need for the test, its risks, how it will be done, or what the results will mean. To help you understand the importance of this procedure, fill out the medical test information form( What is a PDF document? ).
Tell your doctor if you:
- Are taking any medicines.
- Have allergies to any medicines, including anesthetics.
- Take a blood thinner, or if you have had bleeding problems.
- Are or might be pregnant.
Also, certain conditions may increase the difficulty of thoracentesis. Let your doctor know if you have:
- Had lung surgery. The scarring from the first procedure may make it difficult to do this procedure.
- A long-term (chronic), irreversible lung disease, such as emphysema.
A chest X-ray is usually done before the procedure. Your doctor may order certain blood tests, such as a complete blood count (CBC) and clotting factors, before your procedure.
How It Is Done
This procedure may be done in your doctor’s office, in the X-ray department of a hospital, in an emergency room, or at your bedside in the hospital. Your doctor may have a nurse assist with the procedure.
You will need to take off all or most of your clothes (you may be allowed to keep on your underwear if it does not interfere with the procedure). You will be given a cloth or paper covering to use during the procedure. During the procedure, you will be seated but leaning forward on a padded bedside table. If your test is done in the X-ray department, X-rays or an ultrasound may be used to confirm the location of fluid in your chest.
The needle site between your ribs will be cleaned with an antiseptic solution. Your doctor will give you a local anesthetic in your chest wall so you won’t feel any pain when the longer needle that withdraws the fluid is inserted. Once the area is numb, your doctor will insert the needle to where the fluid has collected (pleural space). You may feel some mild pain or pressure as the needle enters the pleural space.
A syringe or a small tube attached to a vacuum bottle is used to remove the pleural fluid. Your doctor will collect fluid to send to the lab. Once the fluid is removed, the needle or small tube is removed and a bandage is put on the site.
This procedure takes about 10 to 15 minutes.
After the test
An X-ray may be taken right after the procedure to make sure that no complications have occurred.
If more pleural fluid collects and needs to be removed, another thoracentesis may be done later.
How It Feels
When you are given the shot to numb your skin at the needle site, you will feel a sharp stinging or burning sensation that lasts a few seconds. When the needle is inserted into the chest wall, you may again feel a sharp pain for a few seconds.
When the pleural fluid is removed, you may feel a sense of “pulling” or pressure in your chest. Tell your doctor or nurse if you feel faint or if you have any shortness of breath, chest pain, or uncontrollable cough.
If a large amount of pleural fluid was removed during the procedure, you will probably be able to breathe more easily.
Risks
Thoracentesis is generally a safe procedure. A chest X-ray may be done right after the procedure to make sure that no complications have occurred. Complications may include:
- A partial collapse of the lung (pneumothorax). This may occur if the needle used to remove the pleural fluid punctures the lung, allowing air to flow into the pleural space.
- Pulmonary edema, which may occur if a large amount of fluid is removed.
- Infection and bleeding.
- Damage to the liver or spleen, though this is rare.
Results
Thoracentesis is a procedure to remove fluid from the space between the lungs and the chest wall called the pleural space. Results from a lab are usually available in 1 to 2 working days. If the fluid is being tested for an infection, such as tuberculosis, results may not be available for several weeks.
|
Normal: |
A small amount of clear, colorless, or pale yellow pleural fluid, usually less than 20 mL (0.7 fl oz), is normally present. No infection, inflammation, or cancer is found. |
|
Abnormal: |
A large amount of pleural fluid is present. |
|
Fluid may be labeled as either a transudate or an exudate. The difference between these two types of fluid has to do with the amount of protein and other substances found in the fluid.
|
What Affects the Test
Reasons you may not be able to have the test or why the results may not be helpful include:
- Use of antibiotics.
- The inability to remain still.
What To Think About
- Thoracentesis may not be done for people who have:
- A bleeding disorder.
- Heart failure or enlargement of the right side of the heart (cor pulmonale).
- A pleural biopsy may be done at the same time as a thoracentesis to collect a sample of tissue from the inner lining of the chest wall.
- Thoracentesis may be done before another procedure called pleurodesis. During this procedure, a chemical or medicine (talc or doxycycline) is put into the pleural space, which triggers an inflammatory reaction over the surface of the lung and inside the pleural space. This in turn causes the layer of pleura attached to the lung to stick to the layer of pleura on the inside of the chest wall. This takes away the space between the pleura and prevents or reduces the collection of more pleural fluid. Pleurodesis may be done when fluid collects in the chest more than one time and the reason for the fluid buildup cannot be corrected.
References
Citations
- Chernecky CC, Berger BJ (2013). Laboratory Tests and Diagnostic Procedures, 6th ed. St. Louis: Saunders.
- Fischbach F, Dunning MB III (2015). A Manual of Laboratory and Diagnostic Tests, 9th ed. Philadelphia: Wolters Kluwer Health.
Other Works Consulted
- Pagana KD, Pagana TJ (2014). Mosby’s Manual of Diagnostic and Laboratory Tests, 5th ed. St. Louis: Mosby.
Current as of: June 9, 2019
Author: Healthwise Staff
Medical Review:Adam Husney, MD – Family Medicine & E. Gregory Thompson, MD – Internal Medicine & David C. Stuesse, MD – Cardiac and Thoracic Surgery

This information does not replace the advice of a doctor. Healthwise, Incorporated, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use. Learn how we develop our content.