Childhood Central Nervous System Embryonal Tumors Treatment (PDQ®): Treatment – Patient Information [NCI]
General Information About Childhood Central Nervous System Embryonal Tumors
Central nervous system (CNS) embryonal tumors may begin in embryonic (fetal) cells that remain in the brain after birth.
Central nervous system (CNS) embryonal tumors form in embryonic cells that remain in the brain after birth. CNS embryonal tumors tend to spread through the cerebrospinal fluid (CSF) to other parts of the brain and spinal cord.
The tumors may be malignant (cancer) or benign (not cancer). Most CNS embryonal tumors in children are malignant. Malignant brain tumors are likely to grow quickly and spread into other parts of the brain. When a tumor grows into or presses on an area of the brain, it may stop that part of the brain from working the way it should. Benign brain tumors grow and press on nearby areas of the brain. They rarely spread to other parts of the brain. Both benign and malignant brain tumors can cause signs or symptoms and need treatment.
Although cancer is rare in children, brain tumors are the second most common type of childhood cancer, after leukemia. This summary is about the treatment of primary brain tumors (tumors that begin in the brain). The treatment of metastatic brain tumors, which begin in other parts of the body and spread to the brain, is not discussed in this summary. For information about the different types of brain and spinal cord tumors, see the PDQ summary on Childhood Brain and Spinal Cord Tumors Treatment Overview.
Brain tumors occur in both children and adults. Treatment for adults may be different from treatment for children. See the PDQ summary on Adult Central Nervous System Tumors Treatment for more information on the treatment of adults.
There are different types of CNS embryonal tumors.
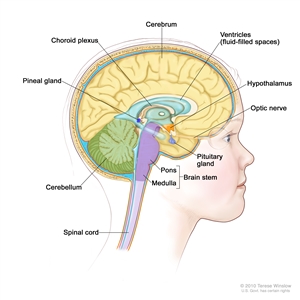
Anatomy of the inside of the brain, showing the pineal and pituitary glands, optic nerve, ventricles (with cerebrospinal fluid shown in blue), and other parts of the brain.
The different types of CNS embryonal tumors include:
| Medulloblastomas
Most CNS embryonal tumors are medulloblastomas. Medulloblastomas are fast-growing tumors that form in brain cells in the cerebellum. The cerebellum is at the lower back part of the brain between the cerebrum and the brain stem. The cerebellum controls movement, balance, and posture. Medulloblastomas sometimes spread to the bone, bone marrow, lung, or other parts of the body, but this is rare. |
| Nonmedulloblastoma embryonal tumors
Nonmedulloblastoma embryonal tumors are fast-growing tumors that usually form in brain cells in the cerebrum. The cerebrum is at the top of the head and is the largest part of the brain. The cerebrum controls thinking, learning, problem-solving, emotions, speech, reading, writing, and voluntary movement. Nonmedulloblastoma embryonal tumors may also form in the brain stem or spinal cord. There are four types of nonmedulloblastoma embryonal tumors:
|
Childhood CNS atypical teratoid/rhabdoid tumor is also a type of embryonal tumor, but it is treated differently than other childhood CNS embryonal tumors. See the PDQ summary on Childhood Central Nervous System Atypical Teratoid/Rhabdoid Tumor Treatment for more information.
Pineoblastomas form in cells of the pineal gland.
The pineal gland is a tiny organ in the center of the brain. The gland makes melatonin, a substance that helps control our sleep cycle.
Pineoblastomas form in cells of the pineal gland and are usually malignant. Pineoblastomas are fast-growing tumors with cells that look very different from normal pineal gland cells. Pineoblastomas are not a type of CNS embryonal tumor but treatment for them is a lot like treatment for CNS embryonal tumors.
Pineoblastoma is linked with inherited changes in the retinoblastoma (RB1) gene. A child with the inherited form of retinoblastoma (cancer than forms in the tissues of the retina) has an increased risk of pineoblastoma. When retinoblastoma forms at the same time as a tumor in or near the pineal gland, it is called trilateral retinoblastoma. MRI (magnetic resonance imaging) testing in children with retinoblastoma may detect pineoblastoma at an early stage when it can be treated successfully.
Certain genetic conditions increase the risk of childhood CNS embryonal tumors.
Anything that increases the risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your child’s doctor if you think your child may be at risk.
Risk factors for CNS embryonal tumors include having the following inherited diseases:
- Turcot syndrome.
- Rubinstein-Taybi syndrome.
- Nevoid basal cell carcinoma (Gorlin) syndrome.
- Li-Fraumeni syndrome.
- Fanconi anemia.
Children with certain gene changes or a family history of cancers linked to changes in the BRCA gene may be considered for genetic testing. Although rare, this is to check whether the child has a cancer predisposition syndrome that places the child at risk for other diseases or types of cancer.
In most cases, the cause of CNS embryonal tumors is not known.
Signs and symptoms of childhood CNS embryonal tumors or pineoblastomas depend on the child’s age and where the tumor is.
These and other signs and symptoms may be caused by childhood CNS embryonal tumors, pineoblastomas, or other conditions. Check with your child’s doctor if your child has any of the following:
- Loss of balance, trouble walking, worsening handwriting, or slow speech.
- Lack of coordination.
- Headache, especially in the morning, or headache that goes away after vomiting.
- Double vision or other eye problems.
- Nausea and vomiting.
- General weakness or weakness on one side of the face.
- Unusual sleepiness or change in energy level.
- Seizures.
Infants and young children with these tumors may be irritable or grow slowly. Also they may not eat well or meet developmental milestones such as sitting, walking, and talking in sentences.
Tests that examine the brain and spinal cord are used to detect (find) childhood CNS embryonal tumors or pineoblastomas.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Neurological exam: A series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks a patient’s mental status, coordination, and ability to walk normally, and how well the muscles, senses, and reflexes work. This may also be called a neuro exam or a neurologic exam.
- MRI (magnetic resonance imaging) of the brain and spinal cord with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the brain and spinal cord. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI). Sometimes magnetic resonance spectroscopy (MRS) is done during the MRI scan to look at the chemicals in brain tissue.
- Lumbar puncture: A procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs of tumor cells. The sample may also be checked for the amounts of protein and glucose. A higher than normal amount of protein or lower than normal amount of glucose may be a sign of a tumor. This procedure is also called an LP or spinal tap.
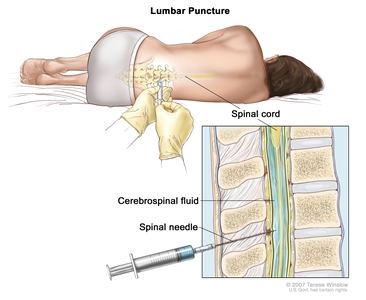
Lumbar puncture. A patient lies in a curled position on a table. After a small area on the lower back is numbed, a spinal needle (a long, thin needle) is inserted into the lower part of the spinal column to remove cerebrospinal fluid (CSF, shown in blue). The fluid may be sent to a laboratory for testing.
A biopsy may be done to be sure of the diagnosis of CNS embryonal tumor or pineoblastoma.
If doctors think your child may have a CNS embryonal tumor or pineoblastoma, a biopsy may be done. For brain tumors, the biopsy is done by removing part of the skull and using a needle to remove a sample of tissue. Sometimes, a computer-guided needle is used to remove the tissue sample. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are found, the doctor may remove as much tumor as safely possible during the same surgery. The piece of skull is usually put back in place after the procedure.
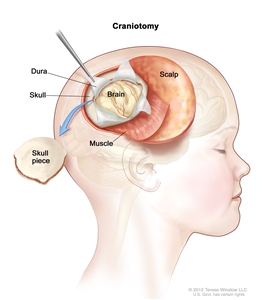
Craniotomy: An opening is made in the skull and a piece of the skull is removed to show part of the brain.
The following test may be done on the sample of tissue that is removed:
- Immunohistochemistry: A test that uses antibodies to check for certain antigens in a sample of tissue. The antibody is usually linked to a radioactive substance or a dye that causes the tissue to light up under a microscope. This type of test may be used to tell the difference between different types of brain tumors.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on:
- The type of tumor and where it is in the brain.
- Whether the cancer has spread within the brain and spinal cord when the tumor is found.
- The age of the child when the tumor is found.
- How much of the tumor remains after surgery.
- Whether there are certain changes in the chromosomes, genes, or brain cells.
- Whether the tumor has just been diagnosed or has recurred (come back).
Staging Childhood Central Nervous System Embryonal Tumors
Treatment of childhood central nervous system (CNS) embryonal tumors and pineoblastomas depends on the type of tumor and the child’s age.
Staging is the process used to find out how much cancer there is and if cancer has spread. It is important to know the stage in order to plan treatment.
There is no standard staging system for childhood central nervous system (CNS) embryonal tumors and pineoblastomas. Instead, treatment depends on the type of tumor and the child’s age (3 years and younger or older than 3 years).
Treatment of medulloblastoma in children older than 3 years also depends on whether the tumor is average risk or high risk.
Average risk (child is older than 3 years of age)
Medulloblastomas are called average risk when all of the following are true:
- The tumor was completely removed by surgery or there was only a very small amount remaining.
- The cancer has not spread to other parts of the body.
High risk (child is older than 3 years of age)
Medulloblastomas are called high risk if any of the following are true:
- Some of the tumor was not removed by surgery.
- The cancer has spread to other parts of the brain or spinal cord or to other parts of the body.
In general, cancer is more likely to recur (come back) in patients with a high-risk tumor.
The information from tests and procedures done to detect (find) childhood CNS embryonal tumors or pineoblastomas is used to plan cancer treatment.
Some of the tests used to detect childhood CNS embryonal tumors or pineoblastomas are repeated after surgery to remove the tumor. (See the General Information section.) This is to find out how much tumor remains after surgery.
Other tests and procedures may be done to find out if the cancer has spread:
- Bone marrow aspiration and biopsy: The removal of bone marrow, blood, and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to look for signs of cancer. A bone marrow aspiration and biopsy is only done when there are signs the cancer has spread to the bone marrow.
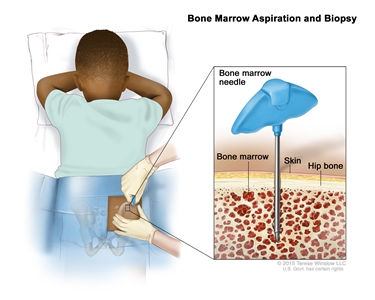
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the child’s hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope. - Bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner. A bone scan is only done when there are signs or symptoms that the cancer has spread to the bone.
- Lumbar puncture: A procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs of tumor cells. The sample may also be checked for the amounts of protein and glucose. A higher than normal amount of protein or lower than normal amount of glucose may be a sign of a tumor. This procedure is also called an LP or spinal tap.
Treatment Option Overview
There are different types of treatment for children who have central nervous system (CNS) embryonal tumors.
Different types of treatment are available for children with central nervous system (CNS) embryonal tumors. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Because cancer in children is rare, taking part in a clinical trial should be considered. Some clinical trials are open only to patients who have not started treatment.
Children who have CNS embryonal tumors should have their treatment planned by a team of health care providers who are experts in treating brain tumors in children.
Treatment will be overseen by a pediatric oncologist, a doctor who specializes in treating children with cancer. The pediatric oncologist works with other pediatric health care providers who are experts in treating children with brain tumors and who specialize in certain areas of medicine. These may include the following specialists:
- Pediatrician.
- Neurosurgeon.
- Neurologist.
- Neuropathologist.
- Neuroradiologist.
- Rehabilitation specialist.
- Radiation oncologist.
- Psychologist.
Childhood brain tumors may cause signs or symptoms that begin before the cancer is diagnosed and continue for months or years.
Signs or symptoms caused by the tumor may begin before the cancer is diagnosed and continue for months or years. It is important to talk with your child’s doctors about signs or symptoms caused by the tumor that may continue after treatment.
Treatment for childhood central nervous system embryonal tumors may cause side effects.
For information about side effects that begin during treatment for cancer, see our Side Effects page.
Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include the following:
- Physical problems.
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer).
Children diagnosed with medulloblastoma may have certain problems after surgery or radiation therapy such as changes in the ability to think, learn, and pay attention. Also, cerebellar mutism syndrome may occur after surgery. Signs of this syndrome include the following:
- Delayed ability to speak.
- Trouble swallowing and eating.
- Loss of balance, trouble walking, and worsening handwriting.
- Loss of muscle tone.
- Mood swings and changes in personality.
Some late effects may be treated or controlled. It is important to talk with your child’s doctors about the effects cancer treatment can have on your child. (See the PDQ summary on Late Effects of Treatment for Childhood Cancer for more information).
Five types of treatment are used:
Surgery
Surgery is used to diagnose and treat a childhood CNS embryonal tumor as described in the General Information section of this summary.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy, radiation therapy, or both after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer. Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. These types of radiation therapy include the following:
- Conformal radiation therapy: Conformal radiation therapy is a type of external radiation therapy that uses a computer to make a 3-dimensional (3-D) picture of the tumor and shapes the radiation beams to fit the tumor. This allows a high dose of radiation to reach the tumor and causes less damage to nearby healthy tissue.
- Stereotactic radiation therapy: Stereotactic radiation therapy is a type of external radiation therapy. A rigid head frame is attached to the skull to keep the head still during the radiation treatment. A machine aims radiation directly at the tumor, causing less damage to nearby healthy tissue. The total dose of radiation is divided into several smaller doses given over several days. This procedure is also called stereotactic external-beam radiation therapy and stereotaxic radiation therapy.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
Radiation therapy to the brain can affect growth and development in young children. For this reason, clinical trials are studying new ways of giving radiation that may have fewer side effects than standard methods.
The way the radiation therapy is given depends on the type of cancer being treated. External radiation therapy is used to treat childhood CNS embryonal tumors.
Because radiation therapy can affect growth and brain development in young children, especially children who are three years old or younger, chemotherapy may be given to delay or reduce the need for radiation therapy.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Combination chemotherapy is treatment using more than one anticancer drug. The way the chemotherapy is given depends on the type of cancer being treated.
Regular dose anticancer drugs given by mouth or vein to treat central nervous system tumors cannot cross the blood-brain barrier and enter the fluid that surrounds the brain and spinal cord. Instead, an anticancer drug is injected into the fluid-filled space to kill cancer cells that may have spread there. This is called intrathecal or intraventricular chemotherapy.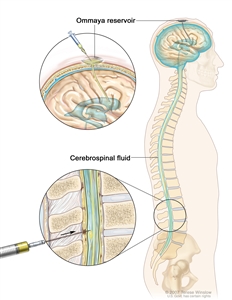
Intrathecal chemotherapy. Anticancer drugs are injected into the intrathecal space, which is the space that holds the cerebrospinal fluid (CSF, shown in blue). There are two different ways to do this. One way, shown in the top part of the figure, is to inject the drugs into an Ommaya reservoir (a dome-shaped container that is placed under the scalp during surgery; it holds the drugs as they flow through a small tube into the brain). The other way, shown in the bottom part of the figure, is to inject the drugs directly into the CSF in the lower part of the spinal column, after a small area on the lower back is numbed.
High-dose chemotherapy with stem cell rescue
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood -forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body’s blood cells.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to attack cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do.
Signal transduction inhibitors are a type of targeted therapy used to treat recurrent medulloblastoma. Signal transduction inhibitors block signals that are passed from one molecule to another inside a cell. Blocking these signals may kill cancer cells. Vismodegib is a type of signal transduction inhibitor.
Targeted therapy is being studied for the treatment of childhood CNS embryonal tumors that have recurred (come back).
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. (See the General Information section for a list of tests.) Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests. This is sometimes called re-staging.
Some of the imaging tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child’s condition has changed or if the brain tumor has recurred (come back). If the imaging tests show abnormal tissue in the brain, a biopsy may also be done to find out if the tissue is made up of dead tumor cells or if new cancer cells are growing. These tests are sometimes called follow-up tests or check-ups.