Pacemaker for Heart Failure (Cardiac Resynchronization Therapy)
Treatment Overview
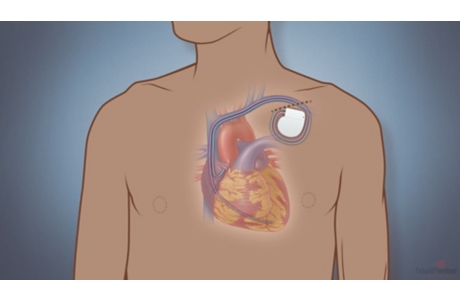
Cardiac resynchronization therapy (CRT) uses a special type of pacemaker called a biventricular pacemaker (say “by-ven-TRICK-yuh-ler”) to treat heart failure. This pacemaker sends electrical pulses to make the ventricles pump at the same time.
A biventricular pacemaker is implanted in the chest, and it connects to three thin wires, called leads. The leads go into different chambers of your heart. If there is a problem with your heartbeat, the pacemaker sends a painless signal through the leads to fix the problem. The pacemaker also can speed up your heart if it is beating too slowly.
In some cases, you may get a pacemaker that is combined with a device to shock your heartbeat back to a normal rhythm if it is dangerously fast. The device is called an implantable cardioverter-defibrillator, or ICD. It can prevent sudden death.
Your doctor will put the pacemaker in your chest during minor surgery. You will not have open-chest surgery.
Your doctor makes a small cut (incision) in your chest. The doctor puts the leads in a vein and threads them to the heart. Then your doctor connects the leads to the pacemaker. Your doctor puts the pacemaker in your chest and closes the incision. Your doctor also programs the pacemaker.
What To Expect
Most people spend the night in the hospital, just to make sure that the device is working and that there are no problems from the surgery. But sometimes the procedure is done as an outpatient procedure, which means you don’t need to stay overnight in the hospital.
You may be able to see a little bump under the skin where the pacemaker is placed.
Daily precautions
Some electric devices have a strong electromagnetic field. This field can keep your pacemaker from working right for a short time. These devices include things in your home, garage, or workplace. Check with your doctor about what you need to avoid and what you need to keep a short distance away from your pacemaker. Many household and office electronics will not affect your pacemaker.
Why It Is Done
When you have heart failure, the lower chambers of your heart (the ventricles) aren’t able to pump as much blood as your body needs. Sometimes the heart has a problem with the electrical system that controls the pumping. This means the ventricles don’t pump at the right time or the heart has an abnormal rhythm. A pacemaker for heart failure can help the heart pump blood better.
Whether a pacemaker for heart failure is right for you depends on many medical facts. Your doctor will check many things including:footnote 1
- How bad your symptoms are and if you have trouble doing everyday activities. Heart failure is grouped—or classified—according to symptoms. Your doctor will probably talk about your heart failure “class” number, which will be between I and IV.
- Your ejection fraction. This is a measure of how much blood your left ventricle pumps.
- Your heart’s electrical system. You will likely have tests to check for heart rhythm problems.
How Well It Works
A pacemaker can help your heart pump blood better. It may help you feel better so you can be more active. It also may help keep you out of the hospital and help you live longer.
A pacemaker can slow the progression of heart failure. It can do this by helping the heart’s electrical system work well and by changing the shape of your heart. In heart failure, the left ventricle often gets too big as it tries to make up for not pumping well. The pacemaker can slow down this change in your ventricle. It might even help your ventricle go back to a more normal size.
- A large study found that 19 out of 100 people who were treated with a pacemaker for heart failure had to go into the hospital during the study because of heart failure. But 27 out of 100 people treated with medicine alone had to go into the hospital for heart failure.footnote 2
- In the same study, 13 out of 100 people who got a pacemaker for heart failure died during the study, compared with 16 out of 100 who got only medicine.footnote 2
- The combination of a pacemaker and an ICD (implantable cardioverter-defibrillator) can also help people live longer and stay out of the hospital.footnote 3
Risks
There are several risks to getting a pacemaker. But risks vary for each person. The chance of most problems is low.
The procedure to implant a pacemaker is safe, and most people do well afterward. Afterward, you will see your doctor regularly to check your pacemaker and make sure you don’t have any problems.
During the procedure
If problems happen during the procedure, doctors likely can fix them right away.
- A lung could collapse (pneumothorax). This happens if air builds up in the space between the lung and the chest wall. But a pneumothorax can be treated and people recover well. This might happen about 1 time out of 100. So about 99 times out of 100, no problems happen.footnote 4
- A tear in the heart could happen. Or a person might need emergency medicine or surgery. Based on rates of complications from patients, these problems happen about 1 time out of 100. So about 99 times out of 100, these problems do not happen.footnote 5
- The pacemaker might not be able to be implanted for several reasons, such as when a vein near the left ventricle is too small, too wide, or too hard to reach to allow a lead to be placed. Sometimes the chest or heart may be too big to place a lead. The chance that a doctor can’t place the pacemaker is about 8 out of 100. That means the pacemaker can be placed 92 times out of 100.footnote 4
After the procedure
Problems after the procedure can be minor, like mild pain, or serious, like an infection. But your doctor can solve most of these problems. And most people do not have long-term issues with their pacemakers.
Problems include:
- Pain, bleeding, or bruising soon after the procedure.
- Infection in your chest near the pacemaker. An infection might happen about 1 time out of 100. This means that about 99 times out of 100 there is no infection.footnote 6
- The pacemaker or leads might not work. This might happen about 7 times out of 100. So 93 times out of 100, the pacemaker and leads do work.footnote 7
- A lead might move out of place. This might happen up to 9 times out of 100. So about 91 out of 100 times, the lead stays in place.footnote 7
What To Think About
Follow your doctor’s specific instructions about care and precautions if you have a pacemaker.
References
Citations
- Yancy CW, et al. (2013). 2013 ACCF/AHA Guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology, 62(16): e147–e239.
- McAlister FA, et al. (2007). Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: A systematic review. JAMA, 297(22): 2502–2514.
- Tang ASL, et al. (2010). Cardiac-resynchronization therapy for mild-to-moderate heart failure. New England Journal of Medicine, 363(25): 2385–2395.
- Van Rees JB, et al. (2011). Implantation-related complications of implantable cardioverter-defibrillators and cardiac resynchronization therapy devices. Journal of the American College of Cardiology, 58(10): 995–1000.
- Poole JE, et al. (2010). Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures. Circulation, 122(16): 1553–1561. DOI: 10.1161/CIRCULATIONAHA.110.976076. Accessed December 15, 2016.
- Baddour LM, et al. (2010). Update on cardiovascular implantable electronic device infections and their management. A scientific statement from the American Heart Association. Circulation, 121(3): 458–477.
- McKelvie R (2011). Heart failure, search date August 2010. BMJ Clinical Evidence. Available online: http://www.clinicalevidence.com.
Other Works Consulted
- Bogale N, et al. (2012). The European CRT survey: 1 year (9–15 months) follow-up results. European Journal of Heart Failure, 14(1): 61–73.
- Lampert R, et al. (2010). HRS Expert Consensus Statement on the Management of Cardiovascular Implantable Electronic Devices (CIEDs) in patients nearing end of life or requesting withdrawal of therapy. Heart Rhythm, 7(7): 1008–1026. Available online: http://www.hrsonline.org/Policy/ClinicalGuidelines/upload/ceids_mgmt_eol.pdf.
Credits
Current as of: April 9, 2019
Author: Healthwise Staff
Medical Review:Rakesh K. Pai MD, FACC – Cardiology, Electrophysiology & Martin J. Gabica MD – Family Medicine & Kathleen Romito MD – Family Medicine & E. Gregory Thompson MD – Internal Medicine & Adam Husney MD – Family Medicine & John M. Miller MD, FACC – Cardiology, Electrophysiology
Current as of: April 9, 2019
Author: Healthwise Staff
Medical Review:Rakesh K. Pai MD, FACC – Cardiology, Electrophysiology & Martin J. Gabica MD – Family Medicine & Kathleen Romito MD – Family Medicine & E. Gregory Thompson MD – Internal Medicine & Adam Husney MD – Family Medicine & John M. Miller MD, FACC – Cardiology, Electrophysiology





This information does not replace the advice of a doctor. Healthwise, Incorporated, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use. Learn how we develop our content.