General Information About Pheochromocytoma and Paraganglioma
Pheochromocytoma and paraganglioma are rare tumors that come from the same type of tissue.
Paragangliomas form in nerve tissue in the adrenal glands and near certain blood vessels and nerves. Paragangliomas that form in the adrenal glands are called pheochromocytomas. Paragangliomas that form outside the adrenal glands are called extra-adrenal paragangliomas. In this summary, extra-adrenal paragangliomas are called paragangliomas.
Pheochromocytomas and paragangliomas may be benign (not cancer) or malignant (cancer).
Pheochromocytoma is a rare tumor that forms in the adrenal medulla (the center of the adrenal gland).
Pheochromocytoma forms in the adrenal glands. There are two adrenal glands, one on top of each kidney in the back of the upper abdomen. Each adrenal gland has two parts. The outer layer of the adrenal gland is the adrenal cortex. The center of the adrenal gland is the adrenal medulla.
Pheochromocytoma is a rare tumor of the adrenal medulla. Usually, pheochromocytoma affects one adrenal gland, but it may affect both adrenal glands. Sometimes there is more than one tumor in one adrenal gland.
The adrenal glands make important hormones called catecholamines. Adrenaline (epinephrine) and noradrenaline (norepinephrine) are two types of catecholamines that help control heart rate, blood pressure, blood sugar, and the way the body reacts to stress. Sometimes a pheochromocytoma will release extra adrenaline and noradrenaline into the blood and cause signs or symptoms of disease. 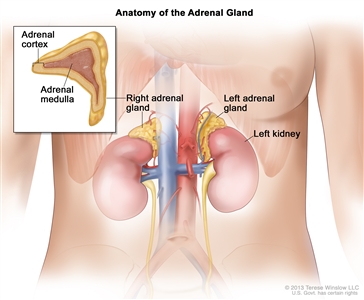
Anatomy of the adrenal gland. There are two adrenal glands, one on top of each kidney. The outer part of each gland is the adrenal cortex; the inner part is the adrenal medulla.
Paragangliomas form outside the adrenal gland.
Paragangliomas are rare tumors that form near the carotid artery, along nerve pathways in the head and neck, and in other parts of the body. Some paragangliomas make extra catecholamines called adrenaline and noradrenaline. The release of these extra catecholamines into the blood may cause signs or symptoms of disease.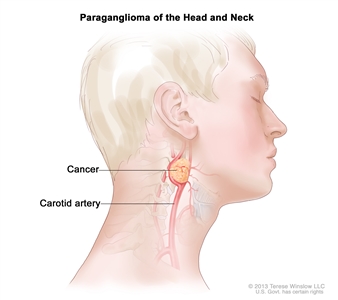
Paraganglioma of the head and neck. A rare tumor that often forms near the carotid artery. It may also form along nerve pathways in the head and neck and in other parts of the body.
Certain inherited disorders and changes in certain genes increase the risk of pheochromocytoma or paraganglioma.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor doesn’t mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk to your doctor if you think you may be at risk.
The following inherited syndromes or gene changes increase the risk of pheochromocytoma or paraganglioma:
- Multiple endocrine neoplasia 2 syndrome, types A and B (MEN2A and MEN2B).
- von Hippel-Lindau (VHL) syndrome.
- Neurofibromatosis type 1 (NF1).
- Hereditary paraganglioma syndrome.
- Carney-Stratakis dyad (paraganglioma and gastrointestinal stromal tumor [GIST]).
- Carney triad (paraganglioma, GIST, and pulmonary chondroma).
Signs and symptoms of pheochromocytoma and paraganglioma include high blood pressure and headache.
Some tumors do not make extra adrenaline or noradrenaline and do not cause signs and symptoms. These tumors are sometimes found when a lump forms in the neck or when a test or procedure is done for another reason. Signs and symptoms of pheochromocytoma and paraganglioma occur when too much adrenaline or noradrenaline is released into the blood. These and other signs and symptoms may be caused by pheochromocytoma and paraganglioma or by other conditions. Check with your doctor if you have any of the following:
- High blood pressure.
- Headache.
- Heavy sweating for no known reason.
- A strong, fast, or irregular heartbeat.
- Being shaky.
- Being extremely pale.
The most common sign is high blood pressure. It may be hard to control. Very high blood pressure can cause serious health problems such as irregular heartbeat, heart attack, stroke, or death.
Signs and symptoms of pheochromocytoma and paraganglioma may occur at any time or be brought on by certain events.
Signs and symptoms of pheochromocytoma and paraganglioma may occur when one of the following events happens:
- Hard physical activity.
- A physical injury or having a lot of emotional stress.
- Childbirth.
- Going under anesthesia.
- Surgery, including procedures to remove the tumor.
- Eating foods high in tyramine (such as red wine, chocolate, and cheese).
Tests that examine the blood and urine are used to detect (find) and diagnose pheochromocytoma and paraganglioma.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as high blood pressure or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Twenty-four-hour urine test: A test in which urine is collected for 24 hours to measure the amounts of catecholamines in the urine. Substances caused by the breakdown of these catecholamines are also measured. An unusual (higher or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. Higher-than-normal amounts of certain catecholamines may be a sign of pheochromocytoma.
- Blood catecholamine studies: A procedure in which a blood sample is checked to measure the amount of certain catecholamines released into the blood. Substances caused by the breakdown of these catecholamines are also measured. An unusual (higher than or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. Higher-than-normal amounts of certain catecholamines may be a sign of pheochromocytoma.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the neck, chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body such as the neck, chest, abdomen, and pelvis. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Genetic counseling is part of the treatment plan for patients with pheochromocytoma or paraganglioma.
All patients who are diagnosed with pheochromocytoma or paraganglioma should have genetic counseling to find out their risk for having an inherited syndrome and other related cancers.
Genetic testing may be recommended by a genetic counselor for patients who:
- Have a personal or family history of traits linked with inherited pheochromocytoma or paraganglioma syndrome.
- Have tumors in both adrenal glands.
- Have more than one tumor in one adrenal gland.
- Have signs or symptoms of extra catecholamines being released into the blood or malignant (cancerous) paraganglioma.
- Are diagnosed before age 40.
Genetic testing is sometimes recommended for patients with pheochromocytoma who:
- Are aged 40 to 50 years.
- Have a tumor in one adrenal gland.
- Do not have a personal or family history of an inherited syndrome.
When certain gene changes are found during genetic testing, the testing is usually offered to family members who are at risk but do not have signs or symptoms.
Genetic testing is not recommended for patients older than 50 years.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- Whether the tumor is benign or malignant.
- Whether the tumor is in one area only or has spread to other places in the body.
- Whether there are signs or symptoms caused by a higher-than-normal amount of catecholamines.
- Whether the tumor has just been diagnosed or has recurred (come back).
Stages of Pheochromocytoma and Paraganglioma
After pheochromocytoma and paraganglioma have been diagnosed, tests are done to find out if the tumor has spread to other parts of the body.
The extent or spread of cancer is usually described as stage. It is important to know whether the cancer has spread in order to plan treatment. The following tests and procedures may be used to determine if the tumor has spread to other parts of the body:
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the neck, chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. The abdomen and pelvis are imaged to detect tumors that release catecholamine. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body such as the neck, chest, abdomen, and pelvis. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- MIBG scan: A procedure used to find neuroendocrine tumors, such as pheochromocytoma and paraganglioma. A very small amount of a substance called radioactive MIBG is injected into a vein and travels through the bloodstream. Neuroendocrine tumor cells take up the radioactive MIBG and are detected by a scanner. Scans may be taken over 1-3 days. An iodine solution may be given before or during the test to keep the thyroid gland from absorbing too much of the MIBG.
- Octreotide scan: A type of radionuclide scan used to find certain tumors, including tumors that release catecholamine. A very small amount of radioactive octreotide (a hormone that attaches to certain tumors) is injected into a vein and travels through the bloodstream. The radioactive octreotide attaches to the tumor and a special camera that detects radioactivity is used to show where the tumors are in the body.
- FDG-PET scan (fluorodeoxyglucose-positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of FDG, a type of radioactive glucose (sugar), is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if pheochromocytoma spreads to the bone, the cancer cells in the bone are actually pheochromocytoma cells. The disease is metastatic pheochromocytoma, not bone cancer.
There is no standard staging system for pheochromocytoma and paraganglioma.
Pheochromocytoma and paraganglioma are described as localized, regional, or metastatic.
Localized pheochromocytoma and paraganglioma
The tumor is found in one or both adrenal glands (pheochromocytoma) or in one area only (paraganglioma).
Regional pheochromocytoma and paraganglioma
Cancer has spread to lymph nodes or other tissues near where the tumor began.
Metastatic pheochromocytoma and paraganglioma
The cancer has spread to other parts of the body, such as the liver, lungs, bone, or distant lymph nodes.
Recurrent Pheochromocytoma and Paraganglioma
Recurrent pheochromocytoma or paraganglioma is cancer that has recurred (come back) after it has been treated. The cancer may come back in the same place or in another part of the body.
Treatment Option Overview
There are different types of treatment for patients with pheochromocytoma or paraganglioma.
Different types of treatments are available for patients with pheochromocytoma or paraganglioma. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment
Patients with pheochromocytoma and paraganglioma that cause signs or symptoms are treated with drug therapy.
Drug therapy begins when pheochromocytoma or paraganglioma is diagnosed. This may include:
- Drugs that keep the blood pressure normal. For example, one type of drug called alpha-blockers stops noradrenaline from making small blood vessels more narrow. Keeping the blood vessels open and relaxed improves blood flow and lowers blood pressure.
- Drugs that keep the heart rate normal. For example, one type of drug called beta-blockers stops the effect of too much noradrenaline and slows the heart rate.
- Drugs that block the effect of extra hormones made by the adrenal gland.
Drug therapy is often given for one to three weeks before surgery.
Six types of standard treatment are used:
Surgery
Surgery to remove pheochromocytoma is usually an adrenalectomy (removal of one or both adrenal glands). During this surgery, the tissues and lymph nodes inside the abdomen will be checked and if the tumor has spread, these tissues may also be removed. Drugs may be given before, during, and after surgery to keep blood pressure and heart rate normal.
After surgery to remove the tumor, catecholamine levels in the blood or urine are checked. Normal catecholamine levels are a sign that all the pheochromocytoma cells were removed.
If both adrenal glands are removed, life-long hormone therapy to replace hormones made by the adrenal glands is needed.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type of cancer being treated and whether it is localized, regional, metastatic, or recurrent. External radiation therapy and 131I-MIBG therapy are used to treat pheochromocytoma.
Pheochromocytoma is sometimes treated with 131I-MIBG, which carries radiation directly to tumor cells. 131I-MIBG is a radioactive substance that collects in certain kinds of tumor cells, killing them with the radiation that is given off. The 131I-MIBG is given by infusion. Not all pheochromocytomas take up 131I-MIBG, so a test is done first to check for this before treatment begins.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Combination chemotherapy is treatment using more than one anticancer drug. The way the chemotherapy is given depends on the type of cancer being treated and whether it is localized, regional, metastatic, or recurrent.
Ablation therapy
Ablation is a treatment to remove or destroy a body part or tissue or its function. Ablation therapies used to help kill cancer cells include:
- Radiofrequency ablation: A procedure that uses radio waves to heat and destroy abnormal cells. The radio waves travel through electrodes (small devices that carry electricity). Radiofrequency ablation may be used to treat cancer and other conditions.
- Cryoablation: A procedure in which tissue is frozen to destroy abnormal cells. Liquid nitrogen or liquid carbon dioxide is used to freeze the tissue.
Embolization therapy
Embolization therapy is a treatment to block the artery leading to the adrenal gland. Blocking the flow of blood to the adrenal glands helps kill cancer cells growing there.
Targeted therapy
Targeted therapy is a treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Targeted therapies are used to treat metastatic and recurrent pheochromocytoma.
Sunitinib (a type of tyrosine kinase inhibitor) is a new treatment being studied for metastatic pheochromocytoma. Tyrosine kinase inhibitor therapy is a type of targeted therapy that blocks signals needed for tumors to grow.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for pheochromocytoma and paraganglioma may cause side effects.
For information about side effects caused by treatment for cancer, see our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests will be needed.
Some of the tests that were done to diagnose the cancer or to find out the extent of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment will be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests.
For patients with pheochromocytoma or paraganglioma that causes symptoms, catecholamine levels in the blood and urine will be checked on a regular basis. Catecholamine levels that are higher than normal can be a sign that the cancer has come back.
For patients with paraganglioma that does not cause symptoms, follow-up tests such as CT, MRI, or MIBG scan should be done every year.
For patients with inherited pheochromocytoma, catecholamine levels in the blood and urine will be checked on a regular basis. Other screening tests will be done to check for other tumors that are linked to the inherited syndrome.
Talk to your doctor about which tests should be done and how often. Patients with pheochromocytoma or paraganglioma need lifelong follow-up.
Treatment Options for Pheochromocytoma and Paraganglioma
For information about the treatments listed below, see the Treatment Option Overview section.
Localized Pheochromocytoma and Paraganglioma
Treatment of localized benign pheochromocytoma or paraganglioma is usually surgery to completely remove the tumor. If the tumor is in the adrenal gland, the entire adrenal gland is removed.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Inherited Pheochromocytoma
In patients with inherited pheochromocytoma linked to multiple endocrine neoplasia (MEN2) or von Hippel-Lindau (VHL) syndrome, tumors often form in both adrenal glands. The tumors are usually benign.
- Treatment for inherited pheochromocytoma that forms in one adrenal gland is surgery to completely remove the gland. This surgery may help patients avoid lifelong steroid hormone replacement therapy and acute adrenal insufficiency.
- Treatment for inherited pheochromocytoma that forms in both adrenal glands or later forms in the remaining adrenal gland may be surgery to remove the tumor and as little normal tissue in the adrenal cortex as possible. This surgery may help patients avoid life-long hormone replacement therapy and health problems due to the loss of hormones made by the adrenal gland.
Regional Pheochromocytoma and Paraganglioma
Treatment of pheochromocytoma or paraganglioma that has spread to nearby organs or lymph nodes is surgery to completely remove the tumor. Nearby organs that the cancer has spread to, such as the kidney, liver, part of a major blood vessel, and lymph nodes, may also be removed.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Metastatic Pheochromocytoma and Paraganglioma
Treatment of metastatic pheochromocytoma or paraganglioma may include the following:
- Surgery to completely remove the cancer, including tumors that have spread to distant parts of the body.
- Palliative therapy, to relieve symptoms and improve the quality of life, including:
- Surgery to remove as much cancer as possible.
- Combination chemotherapy.
- Radiation therapy with 131I-MIBG.
- External radiation therapy to areas (such as bone) where cancer has spread and cannot be removed by surgery.
- Embolization (treatment to block an artery that supplies blood to a tumor).
- Ablation therapy using radiofrequency ablation or cryoablation for tumors in the liver or bone.
- A clinical trial of targeted therapy with a tyrosine kinase inhibitor.
- A clinical trial of internal radiation therapy using a new radioactive substance.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Recurrent Pheochromocytoma and Paraganglioma
Treatment of recurrent pheochromocytoma or paraganglioma may include the following:
- Surgery to completely remove the cancer.
- When surgery to remove the cancer is not possible, palliative therapy to relieve symptoms and improve the quality of life, including:
- Combination chemotherapy.
- Targeted therapy.
- Radiation therapy using 131I-MIBG.
- External radiation therapy to areas (such as bone) where cancer has spread and cannot be removed by surgery.
- Ablation therapy using radiofrequency ablation or cryoablation.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Pheochromocytoma During Pregnancy
For information about the treatments listed below, see the Treatment Option Overview section.
Pregnant women with pheochromocytoma need special care.
Although it is rarely diagnosed during pregnancy, pheochromocytoma can be very serious for the mother and the newborn. Women who have an increased risk of pheochromocytoma should have prenatal testing. Pregnant women with pheochromocytoma should be treated by a team of doctors who are experts in this type of care.
Signs of pheochromocytoma in pregnancy may include any of the following:
- High blood pressure during the first 3 months of pregnancy.
- Sudden periods of high blood pressure.
- High blood pressure that is very hard to treat.
The diagnosis of pheochromocytoma in pregnant women includes testing for catecholamine levels in blood and urine. See the General Information section for a description of these tests and procedures. An MRI can be done to safely find tumors in pregnant women because it does not expose the fetus to radiation.
Treatment of pregnant women with pheochromocytoma may include surgery.
Treatment of pheochromocytoma during pregnancy may include the following:
- Surgery to completely remove the cancer during the second trimester (the fourth through the sixth month of pregnancy).
- Surgery to completely remove the cancer combined with delivery of the fetus by cesarean section.
To Learn More About Pheochromocytoma and Paraganglioma
For more information from the National Cancer Institute about pheochromocytoma and paraganglioma, see the following:
- Pheochromocytoma and Paraganglioma Home Page
- Unusual Cancers of Childhood Treatment
- Cryosurgery in Cancer Treatment: Questions and Answers
- Targeted Cancer Therapies
- Genetic Testing for Inherited Cancer Susceptibility Syndromes
For general cancer information and other resources from the National Cancer Institute, see the following:
- About Cancer
- Staging
- Chemotherapy and You: Support for People With Cancer
- Radiation Therapy and You: Support for People With Cancer
- Coping with Cancer
- Questions to Ask Your Doctor about Cancer
- For Survivors and Caregivers
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of pheochromocytoma and paraganglioma. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Pheochromocytoma and Paraganglioma Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/pheochromocytoma/patient/pheochromocytoma-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389499]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Last Revised: 2019-05-24
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI’s Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.